Pain In The Arch Of The Foot Running
Overview
Your arch, made up of your tarsals and metatarsals, bridges the area between your heel and the ball of the foot. The ball of the foot is formed where the metatarsals meet your toes. It creates the base area that you use to support your weight whenever you lift your heels off the ground, whether you?re walking, running, jumping, or just rising up on your toes. Conditions of these structures can make it very uncomfortable to walk.

Causes
There are many different factors that can cause arch pain. A structural imbalance or an injury to the foot can often be the direct cause. However, most frequently the cause is a common condition called plantar fasciitis. The plantar fascia is a broad band of fibrous tissue located along the bottom surface of the foot that runs from the heel to the forefoot. Excessive stretching of the plantar fascia, usually due to over-pronation (flat feet), causes plantar fasciitis. The inflammation caused by the plantar fascia being stretched away from the heel often leads to pain in the heel and arch areas. The pain is often extreme in the morning when an individual first gets out of bed or after a prolonged period of rest. If this condition is left untreated and strain on the longitudinal arch continues, a bony protrusion may develop, known as a heel spur. It is important to treat the condition promptly before it worsens.
Symptoms
Arch pain symptoms could include any of the following, a dull, constant ache if the ligaments have been stretched, swelling or tenderness in the foot, redness or bruising in the event of a more serious injury, difficulty putting weight on the foot, sharp pain when the foot is turned or manipulated, tenderness when pressure is applied. Because the arch of the foot is such a complex structure, arch pain could be an indicator of several different types of injuries. Chronic illnesses such as arthritis could also cause arch pain, and depending on the cause or source of your pain, you may experience discomfort in a variety of different areas. Ask a doctor if you believe you may have injured your foot arch.
Diagnosis
In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics.
Non Surgical Treatment
Rest from any aggravating activities and apply cold therapy whilst in the acute phase when the foot or ankle is painful and inflamed. Your Doctor may prescribe anti-inflammatory medication to help reduce pain and inflammation. Once the initial pain and inflammation has gone then a full rehabilitation program which includes stretching and strengthening exercises for the foot can begin. Consult a foot specialist, podiatrist or physiotherapist who can assess this and biomechanical problems of the foot. Nerve conduction studies may be done to confirm the diagnosis and indicate the location of the entrapment. An X-ray or MRI may also be useful to determine the presence of any other structures such as cysts, arthritis or a tarsal coalition.

Surgical Treatment
Foot surgery is difficult, especially when large amounts of deformity correction are needed. The ability to bring the foot into a new position may not be lasting, even if everything looks perfect in the operating room. The goal is to provide improved position and function of the foot and ankle. In some patients with very severe deformity, the goal is a foot that functions well in a brace. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Particular complications associated with cavus foot surgery include incomplete correction of deformity, return of deformity and incomplete fusion.
Prevention
Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches.
Stretching Exercises
Gastroc stretch. Stand on the edge of a step. Rise slowly on your toes. Lower yourself slowly as far as you can until you feel a stretch in your calf. Don?t roll your foot inward or outward. Hold for 1-2 seconds. Reps:10-20 (stop before you fatigue). Soleus stretch. Same as above, but start with your knee bent so that you feel a slight stretch in your calf or achilles. Maintain the angle of your knee throughout the stretch. Bicycle stretch. Lie on your side. Keeping your top leg straight, bring your knee toward your nose until you feel a slight stretch in the hamstring. Maintaining this angle at your hip, start pretending you are pedalling a bicycle with the top leg. Make sure you feel a slight stretch each time your knee is straight. Reps: 10-30 for each leg. If you feel any pops or clicks in your hip or back, try raising the top leg a little (making the thighs further apart) to eliminate the popping. Foot Intrinsic Exercises. Assisted metatarsal head raising. Sit in a chair. Find the bumps at the ball of your foot just before your big toe and just before the little toe. These are the first (big toe) and fifth (little toe) metatarsal heads. Place your second and third fingers from one hand under the first metatarsal head, and the second and third fingers from the other hand under the fifth metatarsal head. Now lay the thumbs from each hand in a diagonal across your toes so that they form a right angle meeting at the nail of the second toe. Your hands are now in position to assist your toes. Keep your toes straight, with the toe pads on the floor. Use your fingers to help raise all the metatarsal heads (the ball of your foot). Do not let your toes curl under keep them long. Now relax. Reps 7-10 for each foot. As this exercise gets easier, let your fingers do less of the work until your toes can do the exercise unassisted. This can take up to three weeks. When your strength has improved to this point, you can progress to the following three exercises, which are best done in stocking feet on a slippery floor. Active metatarsal head raising. Stand with your weight on both feet. Raise your metatarsal heads (the ball of your foot) while keeping your toes from curling under and maintaining your heel on the ground. Relax. Reps 6-7. Do one foot at a time. If you do more reps than you are ready for, you may well develop cramping in your foot. I once had a client who thought if seven reps were good, 10 were better. For good measure, she did the 10 reps 10 times in a day, and then she was unable to walk the next day from having used a set of muscles she had never exercised before. Don?t overdo it.
Your arch, made up of your tarsals and metatarsals, bridges the area between your heel and the ball of the foot. The ball of the foot is formed where the metatarsals meet your toes. It creates the base area that you use to support your weight whenever you lift your heels off the ground, whether you?re walking, running, jumping, or just rising up on your toes. Conditions of these structures can make it very uncomfortable to walk.
Causes
There are many different factors that can cause arch pain. A structural imbalance or an injury to the foot can often be the direct cause. However, most frequently the cause is a common condition called plantar fasciitis. The plantar fascia is a broad band of fibrous tissue located along the bottom surface of the foot that runs from the heel to the forefoot. Excessive stretching of the plantar fascia, usually due to over-pronation (flat feet), causes plantar fasciitis. The inflammation caused by the plantar fascia being stretched away from the heel often leads to pain in the heel and arch areas. The pain is often extreme in the morning when an individual first gets out of bed or after a prolonged period of rest. If this condition is left untreated and strain on the longitudinal arch continues, a bony protrusion may develop, known as a heel spur. It is important to treat the condition promptly before it worsens.
Symptoms
Arch pain symptoms could include any of the following, a dull, constant ache if the ligaments have been stretched, swelling or tenderness in the foot, redness or bruising in the event of a more serious injury, difficulty putting weight on the foot, sharp pain when the foot is turned or manipulated, tenderness when pressure is applied. Because the arch of the foot is such a complex structure, arch pain could be an indicator of several different types of injuries. Chronic illnesses such as arthritis could also cause arch pain, and depending on the cause or source of your pain, you may experience discomfort in a variety of different areas. Ask a doctor if you believe you may have injured your foot arch.
Diagnosis
In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics.
Non Surgical Treatment
Rest from any aggravating activities and apply cold therapy whilst in the acute phase when the foot or ankle is painful and inflamed. Your Doctor may prescribe anti-inflammatory medication to help reduce pain and inflammation. Once the initial pain and inflammation has gone then a full rehabilitation program which includes stretching and strengthening exercises for the foot can begin. Consult a foot specialist, podiatrist or physiotherapist who can assess this and biomechanical problems of the foot. Nerve conduction studies may be done to confirm the diagnosis and indicate the location of the entrapment. An X-ray or MRI may also be useful to determine the presence of any other structures such as cysts, arthritis or a tarsal coalition.
Surgical Treatment
Foot surgery is difficult, especially when large amounts of deformity correction are needed. The ability to bring the foot into a new position may not be lasting, even if everything looks perfect in the operating room. The goal is to provide improved position and function of the foot and ankle. In some patients with very severe deformity, the goal is a foot that functions well in a brace. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Particular complications associated with cavus foot surgery include incomplete correction of deformity, return of deformity and incomplete fusion.
Prevention
Strap the arches into the anatomically correct positions with athletic tape and leave them like this for some time. If the fallen arches are an issue with the muscular structure, this may give the muscles an opportunity to strengthen. This is definitely not a fallen arches cure all the time but it can help prevent it more times than not. Ask a doctor or physical therapists to show you how to do this taping. Find shoes that fit. This may require that you get your foot measured and molded to ensure that the shoe will fit. Shoes that are too big, too tight or too short, may not directly cause the fallen arches, but they can assist with the damage to the area. These shoes should have thick cushioning inside and have plenty of room for your toes. Walk without shoes as much as possible. Shoes directly assist with weakening and distorting the arches of the feet so going without shoes can actually help strengthen your arches and prevent fallen arches. Walking on hard and bumpy surfaces barefooted makes the muscles in your feet strengthen in order to prevent injury. It is a coping mechanism by your body. Insert heel cups or insoles into the shoes that you wear the most. Many people wear uncomfortable shoes to work and these are the same shoes that cause their arches the most problems. Inserting the heel cups and insoles into these shoes can prevent fallen arches from occurring. Many people place these inserts into all their shoes to ensure support. Ask a medical professional, either your doctor or a physical therapist, about daily foot exercises that may keep the arches stronger than normal. Many times, you can find exercises and stretches on the Internet on various websites. Curling your toes tightly and rotating your feet will help strengthen your longitudinal arches. Relax your feet and shake them for a minute or so before you do any arch exercises. This will loosen the muscles in your feet that stay tight due to normal daily activities. Wear rigid soled sandals whenever possible to provide a strong support for your arches. Wooden soled sandals are the best ones if available. Walk or jog on concrete as much as you can. This will create a sturdy support for your arches. Running or walking in sandy areas or even on a treadmill, does not give rigid support. Instead, these surfaces absorb the step, offering no support for arches.
Stretching Exercises
Gastroc stretch. Stand on the edge of a step. Rise slowly on your toes. Lower yourself slowly as far as you can until you feel a stretch in your calf. Don?t roll your foot inward or outward. Hold for 1-2 seconds. Reps:10-20 (stop before you fatigue). Soleus stretch. Same as above, but start with your knee bent so that you feel a slight stretch in your calf or achilles. Maintain the angle of your knee throughout the stretch. Bicycle stretch. Lie on your side. Keeping your top leg straight, bring your knee toward your nose until you feel a slight stretch in the hamstring. Maintaining this angle at your hip, start pretending you are pedalling a bicycle with the top leg. Make sure you feel a slight stretch each time your knee is straight. Reps: 10-30 for each leg. If you feel any pops or clicks in your hip or back, try raising the top leg a little (making the thighs further apart) to eliminate the popping. Foot Intrinsic Exercises. Assisted metatarsal head raising. Sit in a chair. Find the bumps at the ball of your foot just before your big toe and just before the little toe. These are the first (big toe) and fifth (little toe) metatarsal heads. Place your second and third fingers from one hand under the first metatarsal head, and the second and third fingers from the other hand under the fifth metatarsal head. Now lay the thumbs from each hand in a diagonal across your toes so that they form a right angle meeting at the nail of the second toe. Your hands are now in position to assist your toes. Keep your toes straight, with the toe pads on the floor. Use your fingers to help raise all the metatarsal heads (the ball of your foot). Do not let your toes curl under keep them long. Now relax. Reps 7-10 for each foot. As this exercise gets easier, let your fingers do less of the work until your toes can do the exercise unassisted. This can take up to three weeks. When your strength has improved to this point, you can progress to the following three exercises, which are best done in stocking feet on a slippery floor. Active metatarsal head raising. Stand with your weight on both feet. Raise your metatarsal heads (the ball of your foot) while keeping your toes from curling under and maintaining your heel on the ground. Relax. Reps 6-7. Do one foot at a time. If you do more reps than you are ready for, you may well develop cramping in your foot. I once had a client who thought if seven reps were good, 10 were better. For good measure, she did the 10 reps 10 times in a day, and then she was unable to walk the next day from having used a set of muscles she had never exercised before. Don?t overdo it.
Partial Achilles Tendon Rupture Exercises
Overview 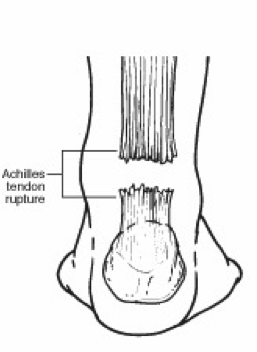 The Achilles tendon is the confluence of the independent tendons of the gastrocnemius and soleus, which fuse to become the Achilles tendon approximately 5 to 6 cm proximal to its insertion on the posterior surface of the calcaneus. The gastrocnemius and soleus muscles, via the Achilles tendon, function as the chief plantarflexors of the ankle joint. This musculotendinous unit provides the primary propulsive force for walking, running, and jumping. The normal Achilles tendon can withstand repetitive loads near its ultimate tensile strength, which approach 6 to 8 times body weight. Causes Common causes of an Achilles tendon rupture include the progression of or the final result of longstanding Achilles tendonitis or an overuse injury. An injury to the ankle or a direct blow to the Achilles tendon. As a result of a fall where an individual lands awkwardly or directly on the ankle. Laceration of the tendon. Weakness of the gastrocnemius or soleus muscles in people with existing Achilles tendonitis places increased stress on the tendon. Steroid use has been linked to tendon weakness. Certain systemic diseases have been associated with tendon weakness. A sudden deceleration or stopping motions that cause an acute traumatic injury of the ankle. Injection of steroids to the involved tendon or the excessive use of steroids has been known to weaken tendons and make them susceptible to rupture. Contraction of the calf muscles while the foot is dorsiflexed (pointed toward the head) and the lower leg is moving forward. Symptoms A classic sign of an Achilles tendon rupture is the feeling of being hit in the Achilles are. There is often a "pop" sound. There may be little pain, but the person can not lift up onto his toes while weight bearing. Diagnosis The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson?s test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected. Non Surgical Treatment This condition should be diagnosed and treated as soon as possible, because prompt treatment probably improves recovery. You may need to be referred urgently to see a doctor in an orthopaedic department or accident and emergency department. Meanwhile, if a ruptured Achilles tendon is suspected, you should not put any weight on that foot, so do not walk on it at all.Treatment options for an Achilles tendon rupture include surgical and non-surgical approaches. The decision of whether to proceed with surgery or non-surgical treatment is based on the severity of the rupture and the patient?s health status and activity level. Non-surgical treatment, which is generally associated with a higher rate of re-rupture, is selected for minor ruptures, less active patients, and those with medical conditions that prevent them from undergoing surgery. Non-surgical treatment involves use of a cast, walking boot, or brace to restrict motion and allow the torn tendon to heal.
The Achilles tendon is the confluence of the independent tendons of the gastrocnemius and soleus, which fuse to become the Achilles tendon approximately 5 to 6 cm proximal to its insertion on the posterior surface of the calcaneus. The gastrocnemius and soleus muscles, via the Achilles tendon, function as the chief plantarflexors of the ankle joint. This musculotendinous unit provides the primary propulsive force for walking, running, and jumping. The normal Achilles tendon can withstand repetitive loads near its ultimate tensile strength, which approach 6 to 8 times body weight. Causes Common causes of an Achilles tendon rupture include the progression of or the final result of longstanding Achilles tendonitis or an overuse injury. An injury to the ankle or a direct blow to the Achilles tendon. As a result of a fall where an individual lands awkwardly or directly on the ankle. Laceration of the tendon. Weakness of the gastrocnemius or soleus muscles in people with existing Achilles tendonitis places increased stress on the tendon. Steroid use has been linked to tendon weakness. Certain systemic diseases have been associated with tendon weakness. A sudden deceleration or stopping motions that cause an acute traumatic injury of the ankle. Injection of steroids to the involved tendon or the excessive use of steroids has been known to weaken tendons and make them susceptible to rupture. Contraction of the calf muscles while the foot is dorsiflexed (pointed toward the head) and the lower leg is moving forward. Symptoms A classic sign of an Achilles tendon rupture is the feeling of being hit in the Achilles are. There is often a "pop" sound. There may be little pain, but the person can not lift up onto his toes while weight bearing. Diagnosis The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson?s test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected. Non Surgical Treatment This condition should be diagnosed and treated as soon as possible, because prompt treatment probably improves recovery. You may need to be referred urgently to see a doctor in an orthopaedic department or accident and emergency department. Meanwhile, if a ruptured Achilles tendon is suspected, you should not put any weight on that foot, so do not walk on it at all.Treatment options for an Achilles tendon rupture include surgical and non-surgical approaches. The decision of whether to proceed with surgery or non-surgical treatment is based on the severity of the rupture and the patient?s health status and activity level. Non-surgical treatment, which is generally associated with a higher rate of re-rupture, is selected for minor ruptures, less active patients, and those with medical conditions that prevent them from undergoing surgery. Non-surgical treatment involves use of a cast, walking boot, or brace to restrict motion and allow the torn tendon to heal.  Surgical Treatment Surgery may be indicated directly following injury rather than conservative care. Repair of an achilles tendon rupture is greatly varied for each clinical situation. There may be a direct repair of the ends of the tendon with suture, or possibly a tendon graft used to augment the tendon. Post-operatively, the period of immobilization will depend on the size of the defect that was repaired and how it was completed. Usually the immobilization is between 6-10 weeks. This repair may allow for a complete return to normal function, but in many instances the healing is complicated with adhesions and a partial loss of range of motion. There may be a continued soft tissue defect noted and a permanent or prolonged swelling.
Surgical Treatment Surgery may be indicated directly following injury rather than conservative care. Repair of an achilles tendon rupture is greatly varied for each clinical situation. There may be a direct repair of the ends of the tendon with suture, or possibly a tendon graft used to augment the tendon. Post-operatively, the period of immobilization will depend on the size of the defect that was repaired and how it was completed. Usually the immobilization is between 6-10 weeks. This repair may allow for a complete return to normal function, but in many instances the healing is complicated with adhesions and a partial loss of range of motion. There may be a continued soft tissue defect noted and a permanent or prolonged swelling.